Treatment of Macular Degeneration and Diabetes is more effective than ever.
2701 North Causeway Boulevard, Metairie, Louisiana 70002, United States

Treatment of Macular Degeneration and Diabetes is more effective than ever.
It can be useful to think of the eye as a camera to understand retinal disease. In this analogy, the lens of the camera is the optical media of the eye including the cornea and lens in the front of the eye. The film of the camera is the retina in the back of the eye.
Retinal detachments occur at rate of about 5 per 100,000 people per year and over a lifetime, one has about a 1 in 300 chance of developing a retinal detachment. Although this disorder is not uncommon, it is a challenging one for those afflicted, because the retina is brain tissue within the eye and does not remain healthy when detached. For this reason, retinal detachment repair is time sensitive.
There are a few types of retinal detachment, including rhegmatogenous, tractional, and serous. The most common type is rhegmatogenous which essentially means that the retinal detachment has resulted from compromise in the retinal tissue which allows subretinal fluid to accumulate. This fluid dissects off the retinal tissue from the wall of the eye.
In understanding retinal detachments, it is useful to picture the retina as wallpaper lining the inside of the sphere that is the eye. In rhegmatogenous detachments, most frequently a tear or hole develops in the retinal wallpaper, which then allows fluid from the center cavity in the eye (fluid inside the sphere) to seep through the hole in the retinal wallpaper. This fluid then dissects off the retinal wallpaper from the wall of the eye just as air under wallpaper prevents wallpaper from laying flat.
The integrity of the retina relies upon the retina laying flat against the wall of the eye because the retina relies on components in the wall of the eye to stay healthy. One of the greatest struggles in retinal detachment pathophysiology is the developement of scar tissue known as proliferative vitreoretinopathy (PVR) which can pull on the retina and re-detach it even after successful retinal detachment repair.
Retina detachment repair techniques in the office include laser, pneumatic retinopexy, and less often cryotherapy. In the simplest terms pneumatic retinopexy involves the injection of gas into the eye to steam roller the retina flat and to use the surface tension of the gas bubble to seal the retinal hole or tear in the hopes that subretinal fluid will resorb and no new fluid will seep in. Once the retina is flatter, laser or cryotherapy are applied with the hopes of tack-welding the retina to the wall behind it in an effort to prevent re-detachment.
Retina detachment repair in the operating room includes most often pars plana vitrectomy (PPV) and scleral buckle techniques. Vitrectomy involves the removal of the vitreous gel in the eye using fine instrumentation under micro-surgical technique. The reason for this is that the natural vitreous gel is often responsible for the mechanical traction on the retina that results in tears and subsequent detachment. Sceral buckles are an entirely different technique in which an external band or other material is applied around the eye to push the wall of the eye inward toward the detached retina. Theories behind the use of buckles include reducing vitreous traction on the retina and blocking retinal tears by apposing the wall of the eye to the tear.
The most common issues in the care of retinal detachments arise when patients think of retinal detachments as a standard disorder with a simple treatment. Because the retina is a living and dynamic brain tissue in the eye, repair of retinal detachment is not as simple as more mechanical approaches to tissue repair. The retina is sensitive to damage from manipulation and scar tissue forms when the retina detaches, which once seeded can potentially re-detach retina for the rest of the patient’s life. Still, most patients have an 80-90% chance of successful re-attachment of the retina after suffering detachment. It should be understood however, that retinal function may not fully return even after successful anatomic retinal detachment repair.

Retinal Detachment
Proliferative Vitreoretinopathy and Giant Retinal Tears
Proliferative vitreoretinopathy (PVR) is a condition in which retinal scar tissue, or “membranes” form; this may occur with a retinal detachment. A key risk factor for developing PVR is a giant retinal tear—a large tear that involves at least 25% of the retina. When PVR or a giant retinal tear is present, a retinal detachment is classified as “complex.”
Many patients with PVR report symptoms of retinal traction (pulling), such as floaters or flashes of light. Accumulation of fluid underneath the retina results in a loss of peripheral (side) vision.
When the detachment involves the center of the retina, called the macula, central vision loss will occur. Patients with chronic retinal detachment may also develop problems such as elevated pressure in the eye and inflammation.
Some patients experience no symptoms, particularly:
But, most often, patients will have some visual symptoms.
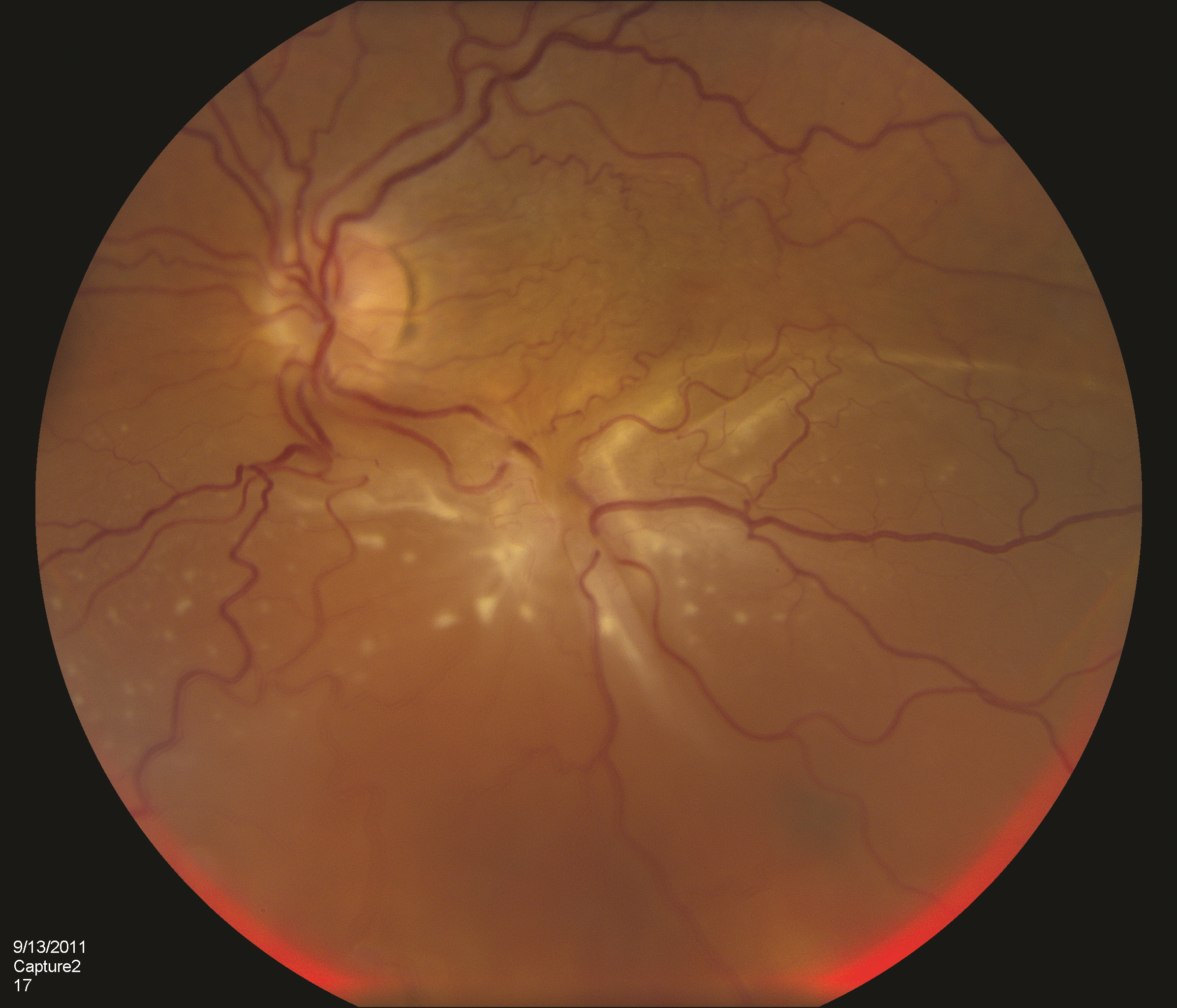
Complex retinal detachments due to PVR are associated with retinal scar tissue or membranes; these ultimately contract, pull, and stretch the retina, causing retinal tears or stretch holes. When the detached retina contracts, so-called “star folds” often develop (Figure 1).
Figure 1. A patient with complex retinal detachment due to PVR in the left eye. A retinal “star fold” is present in the inferior macular with associated subretinal fluid. (Photo courtesy Carl Regillo, MD)
The reason these membranes form is uncertain, but it is thought to be due to cells growing on the retinal surface. Passage of liquefied vitreous gel through a retinal tear or hole results in an accumulation of fluid under the retina (subretinal fluid) and progression of the retinal detachment.
PVR most commonly occurs after a previous (primary) retinal detachment repair surgery. PVR is the most common cause of primary retinal detachment surgery failure, occurring in approximately 5% to 10% of all retinal detachments. Retinal detachment with a giant retinal tear, however, is relatively uncommon.
Many risk factors for PVR have been identified, including:
Viewing the retina with an indirect ophthalmoscope while the doctor applies gentle pressure to the eye (scleral depression) is the primary method for diagnosing retinal detachment. When view of the retina is obscured (blocked) by blood or dense cataract, B-scan ultrasonography can be used to determine the location and extent of a retinal detachment (Figure 2). To confirm whether there is subretinal fluid in the macula, optical coherence tomography (OCT) may be used.
Figure 2. B-scan ultrasound of a patient with PVR-related retinal detachment. A fixed retinal fold (yellow arrow) is seen with a cone-shaped retinal detachment. (Photo courtesy of Yale Fisher, MD. Retina Image Bank, © American Society of Retina Specialists.)
The only treatment option for complex retinal detachment is retinal surgery. Patients may undergo pars plana vitrectomy with peeling of membranes, a scleral buckling procedure, or both. Use of special retinal detachment repair strategies, including retinectomy or perfluorocarbon liquid, may be necessary in patients with complex retinal detachments.
Laser is also used in combination with the vitrectomy to seal the retinal breaks. Your surgeon will decide which procedure is best depending on the nature of your detachment. At the end of surgery, most patients with complex retinal detachment due to PVR or a giant retinal tear will receive a long-acting gas bubble or silicone oil filling into the vitreous cavity of the eye to hold the retina in position while the eye heals.
Research is being conducted to find a medical therapy to prevent and treat PVR, but to date, none has proven effective in most patients.
THANK YOU TO THE RETINA HEALTH SERIES AUTHORS
Sophie J. Bakri, MD Audina Berrocal, MD Antonio Capone, Jr., MDNetan Choudhry, MD, FRCS-CThomas Ciulla, MD, MBA Pravin U. Dugel, MDGeoffrey G. Emerson, MD, PhDRoger A. Goldberg, MD, MBADarin R. Goldman, MD
Dilraj S. Grewal, MD
Larry Halperin, MDVincent S. Hau, MD, PhDSuber S. Huang, MD, MBAMark S. Humayun, MD, PhD Peter K. Kaiser, MDM. Ali Khan, MDAnat Loewenstein, MD Mathew J. MacCumber, MD, PhDMaya Maloney, MDHossein Nazari, MD Oded Ohana, MD, MBAGeorge Parlitsis, MD Jonathan L. Prenner, MDGilad Rabina, MDCarl D. Regillo, MD, FACSAndrew P. Schachat, MD
Michael Seider, MD
Eduardo Uchiyama, MD Allen Z. Verne, MDYoshihiro Yonekawa, MD
EDITOR
John T. Thompson, MD
MEDICAL ILLUSTRATOR
Tim Hengst
Copyright 2016 The Foundation of the American Society of Retina Specialists. All rights reserved.

Vitrectomy surgery for complex retinal detachment
{kind=link}